Allergic Reaction
Recognize
- Itching, hives, flushing, angioedema
- Coughing, wheezing, stridor, or respiratory distress
- Chest or throat constriction
- Difficulty swallowing
- Difficulty phonating
- Nausea / vomiting
- Altered Mental Status
- Hypotension or shock
- Edema
Evaluate
- Onset and trajectory of symptoms
- Anatomic and situational location of exposure
- Insect sting or bite
- Known allergies: food, environmental, medication, other
- Known or suspected exposure: past occurrences and current event
- Known history of sensitivity or allergic reaction
- Past medical and medication history
- New clothing, soap, or detergent
- New medications
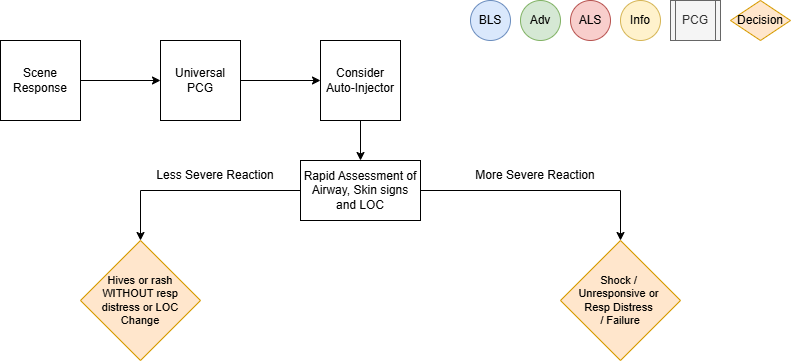
Administer Treatment
- Remove allergy trigger if known and present
- Prioritize interventions based on clinical presentation and severity of reaction
- Supplemental oxygen PRN for goal SpO2
- Attentive and prompt airway assessment and management
Airway Management if indicated per Airway Management PCG (P1)
- If patient has suspected or known exposure and exhibits signs of any: respiratory distress, airway
restriction, altered mental status or shock, treat accordingly
-
- Epinephrine Auto-Injector 0.3 mg IM if available
- Vascular access per Vascular Access PCG (P33)
- Consider crystalloid fluid bolus 500 mL IV/IO to support hemodynamics, repeat PRN
- Diphenhydramine (Benadryl) 50 mg IM/IV/IO
- Epinephrine (1mg/1mL) 0.3 mg IM or Epinephrine (1mg/10mL) 0.1 mg IV/IO q 3 min PRN for
MORE SEVERE REACTION
-
- Consider Epinephrine infusion 0.01 mcg/kg/min IV/IO, titrate to max 0.1 mcg/kg/min
as an alternative to repeat IM or IV/IO doses
- Monitor ECG rhythm closely, Epinephrine may potentiate arrhythmias, especially in
patients over the age of 40
- Methylprednisolone (Solu-Medrol) 125 mg IV/IO
- Albuterol (2.5 mg/3 mL) nebulized for wheezing or shortness of breath
Consider Differentials
Administer Treatment
- Remove allergy trigger if known and present
- Prioritize interventions based on clinical presentation and severity of reaction
- Supplemental oxygen PRN for goal SpO2
- Attentive and prompt airway assessment and management
Airway Management if indicated per Airway Management PCG (P1) - If patient has suspected or known exposure and exhibits signs of any: respiratory distress, airway
restriction, altered mental status or shock, treat accordingly-
- Epinephrine Auto-Injector 0.3 mg IM if available
- Vascular access per Vascular Access PCG (P33)
- Consider crystalloid fluid bolus 500 mL IV/IO to support hemodynamics, repeat PRN
- Diphenhydramine (Benadryl) 50 mg IM/IV/IO
- Epinephrine (1mg/1mL) 0.3 mg IM or Epinephrine (1mg/10mL) 0.1 mg IV/IO q 3 min PRN for
MORE SEVERE REACTION-
- Consider Epinephrine infusion 0.01 mcg/kg/min IV/IO, titrate to max 0.1 mcg/kg/min
as an alternative to repeat IM or IV/IO doses - Monitor ECG rhythm closely, Epinephrine may potentiate arrhythmias, especially in
patients over the age of 40
- Consider Epinephrine infusion 0.01 mcg/kg/min IV/IO, titrate to max 0.1 mcg/kg/min
-
- Methylprednisolone (Solu-Medrol) 125 mg IV/IO
- Albuterol (2.5 mg/3 mL) nebulized for wheezing or shortness of breath
-
Consider Differentials
(rash only)
Transport Considerations
transport, maintain astute airway, breathing, circulation and mental status assessment with
prompt intervention as needed. Stability can quickly change to instability in these patients.
Information
the shorter the interval from exposure to symptoms, the more severe the reaction
Other Populations
Neonatal/ Pediatric drug dosing:
-
- Pediatric Epinephrine Auto-Injector JR dose is 0.15 mg for patients 15-30 Kg
- Diphenhydramine (Benadryl) 1 mg/Kg IM/IV/IO over 5 min max dose 50 mg
- Epinephrine (1mg/1mL) 0.01 mg/Kg IM/IV/IO q3 min until stable or infusion started
-
- Max 0.5 mg per dose (Intentionally larger than adult dosing)
- Epinephrine infusion 0.01 mcg/Kg/min IV/IO, titrate to max 1 mcg/kg/min
- Methylprednisolone (Solu-Medrol) 2 mg/Kg IV/IO max dose 125mg
- Albuterol for 15 Kg or more, use adult dose
- Albuterol for less than 15 Kg (1.25mg/ 3ml) nebulized with O2 at 6 lpm
- Pediatric Epinephrine Auto-Injector JR dose is 0.15 mg for patients 15-30 Kg
- Diphenhydramine (Benadryl) 1 mg/Kg IM/IV/IO over 5 min max dose 50 mg
- Epinephrine (1mg/1mL) 0.01 mg/Kg IM/IV/IO q3 min until stable or infusion started
-
- Max 0.5 mg per dose (Intentionally larger than adult dosing)
- Epinephrine infusion 0.01 mcg/Kg/min IV/IO, titrate to max 1 mcg/kg/min
-
- Methylprednisolone (Solu-Medrol) 2 mg/Kg IV/IO max dose 125mg
- Albuterol for 15 Kg or more, use adult dose
- Albuterol for less than 15 Kg (1.25mg/ 3ml) nebulized with O2 at 6 lpm
Navigate
References
Campbell, Ronna. “Anaphylaxis: Emergency Treatment.” UpToDate, January 2022.
Sicherer, Scott. “Prescribing Epinephrine for Anaphylaxis Self-Treatment.” UpToDate, January 2022.
“U.S. Army Medevac Critical Care Flight Paramedic Standard Medical Operating Guidelines.” Jan. 2020.