Bag-Valve Mask
THIS PROCEDURE APPLIES TO: Any patient unable to adequately ventilate him/herself who needs supplemental oxygen delivered via a bag-valve mask.
EXCLUSION CRITERIA: None
PROCEDURE
- Observe body substance isolation precautions.
- Rescuer 1 should position him/herself at the top of the victim’s head. Rescuer 2 should kneel at the patient’s side.
- Open the patient’s airway and maintain it with an oropharyngeal airway.
- Because bag-valve masks are most effective when used by at least two rescuers working together, when two rescuers are available the bag-valve mask will be a two-person skill.
- When two persons use the bag-valve mask:
- Rescuer 1, using both hands, positions the mask to maintain a seal around the nose and mouth.
- Rescuer 2 squeezes the bag with both hands, delivering each breath over 2 seconds.
- Apply cricoid pressure throughout the entire procedure or until the patient is successfully intubated.
- If only one rescuer is available:
- With one hand, apply the mask to the patient’s face.
- Grip the mandible with the last two or three fingers while gripping the mask with the remaining fingers.
- Maintain head tilt and jaw lift while maintaining a seal around the nose and mouth.
- Compress the bag with the other hand while observing the chest to ensure chest rise.
- Connect the bag-valve mask to an oxygen source.
Ventilating the Conscious Patient
- To avoid resistance or combativeness due to fear, explain the procedure to the patient.
- Begin by matching the volume and rate of the patient’s ineffective breathing. Adjust the rate and volume until you are ventilating at the necessary rate and volume.
Ventilating During CPR
- Administer each ventilation over one second, regardless of the patient’s size or age.
- Each ventilation should be of sufficient volume to make the patient’s chest rise.
- Ventilations administered during CPR increase pressure in the chest. This pressure reduces the amount of blood that refills the heart and in turn reduces the blood flow generated by the next set of chest compressions. For these reasons, ventilating too frequently or with too large a volume (hyperventilating) may be harmful because it may reduce blood flow generated by chest compressions.
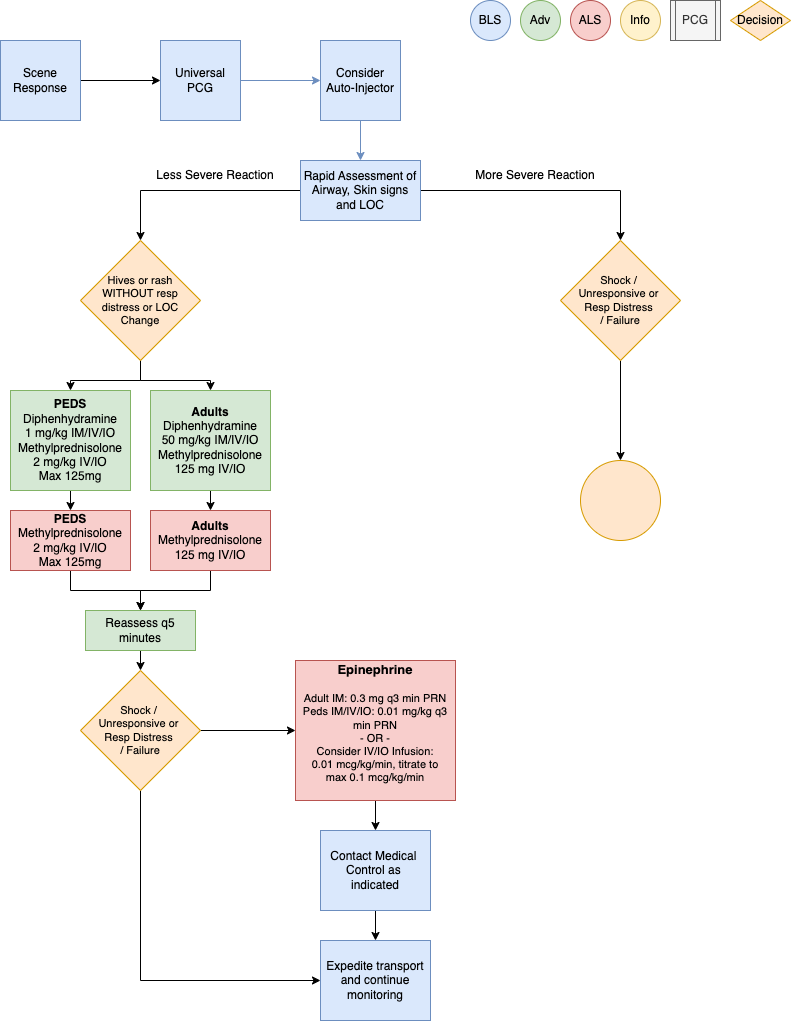
This policy applies to: Patients whose chief complaint is itching, rash or allergic reaction.
Exclusion Criteria: None
Recognize
Itching, hives, flushing, angioedemaCoughing, wheezing, stridor, or respiratory distressChest or throat constrictionDifficulty swallowingDifficulty phonatingNausea / vomitingAltered Mental StatusHypotension or shockEdema
Evaluate
Onset and trajectory of symptomsAnatomic and situational location of exposureInsect sting or biteKnown allergies: food, environmental, medication, otherKnown or suspected exposure: past occurrences and current eventKnown history of sensitivity or allergic reactionPast medical and medication historyNew clothing, soap, or detergentNew medications
Administer Treatment
Remove allergy trigger if known and presentPrioritize interventions based on clinical presentation and severity of reactionSupplemental oxygen PRN for goal SpO2Attentive and prompt airway assessment and managementAirway Management if indicated perAirway Management PCG (P1)If patient has suspected or known exposure and exhibits signs of any: respiratory distress, airwayrestriction, altered mental status or shock, treat accordinglyEpinephrine Auto-Injector 0.3 mg IMif availableVascular access per Vascular Access PCG (P33)Considercrystalloid fluid bolus 500 mL IV/IOto support hemodynamics, repeat PRNDiphenhydramine (Benadryl) 50 mg IM/IV/IOEpinephrine(1mg/1mL)0.3 mg IM or Epinephrine(1mg/10mL)0.1 mg IV/IOq 3 min PRN forMORE SEVERE REACTIONConsiderEpinephrine infusion 0.01 mcg/kg/min IV/IO, titrate to max 0.1 mcg/kg/minas an alternative to repeat IM or IV/IO dosesMonitor ECG rhythm closely, Epinephrine may potentiate arrhythmias, especially inpatients over the age of 40
Methylprednisolone (Solu-Medrol) 125 mg IV/IOAlbuterol (2.5 mg/3 mL) nebulizedfor wheezing or shortness of breath
Consider Differentials
Urticaria (rash only)Anaphylaxis (severe systemic effect)Shock (severe vascular effect)Angioedema (drug induced or infection)Aspiration / airway obstructionVasovagal eventAsthma or COPDInfection (ex: retropharyngeal abscess, bacterial tracheitis, croup, epiglottitis, strep)Pulmonary edema or CHFMetabolic disorders
Transport Considerations
During transport, maintain astute airway, breathing, circulation and mental status assessment withprompt intervention as needed. Stability can quickly change to instability in these patients.Consider early airway management, reference Airway Management PCG (P1)
Information
Typically, the shorter the interval from exposure to symptoms, the more severe the reactionHemodynamic instability may recur up to 24 hours after initial stabilization
Other Populations
Neonatal/ Pediatric drug dosing:PediatricEpinephrine Auto-Injector JR dose is 0.15 mgfor patients 15-30 KgDiphenhydramine (Benadryl) 1 mg/Kg IM/IV/IOover 5 min max dose 50 mgEpinephrine(1mg/1mL)0.01 mg/Kg IM/IV/IOq3 min until stable or infusion startedMax 0.5 mg per dose (Intentionally larger than adult dosing)Epinephrine infusion 0.01 mcg/Kg/min IV/IO, titrate to max 1 mcg/kg/min
Methylprednisolone (Solu-Medrol) 2 mg/Kg IV/IOmax dose 125mgAlbuterol for 15 Kg or more, use adult doseAlbuterol for less than 15 Kg (1.25mg/ 3ml) nebulizedwith O2 at 6 lpm
Navigate
References
Campbell, Ronna. “Anaphylaxis: Emergency Treatment.” UpToDate, January 2022.Sicherer, Scott. “Prescribing Epinephrine for Anaphylaxis Self-Treatment.” UpToDate, January 2022.“U.S. Army Medevac Critical Care Flight Paramedic Standard Medical Operating Guidelines.” Jan. 2020.