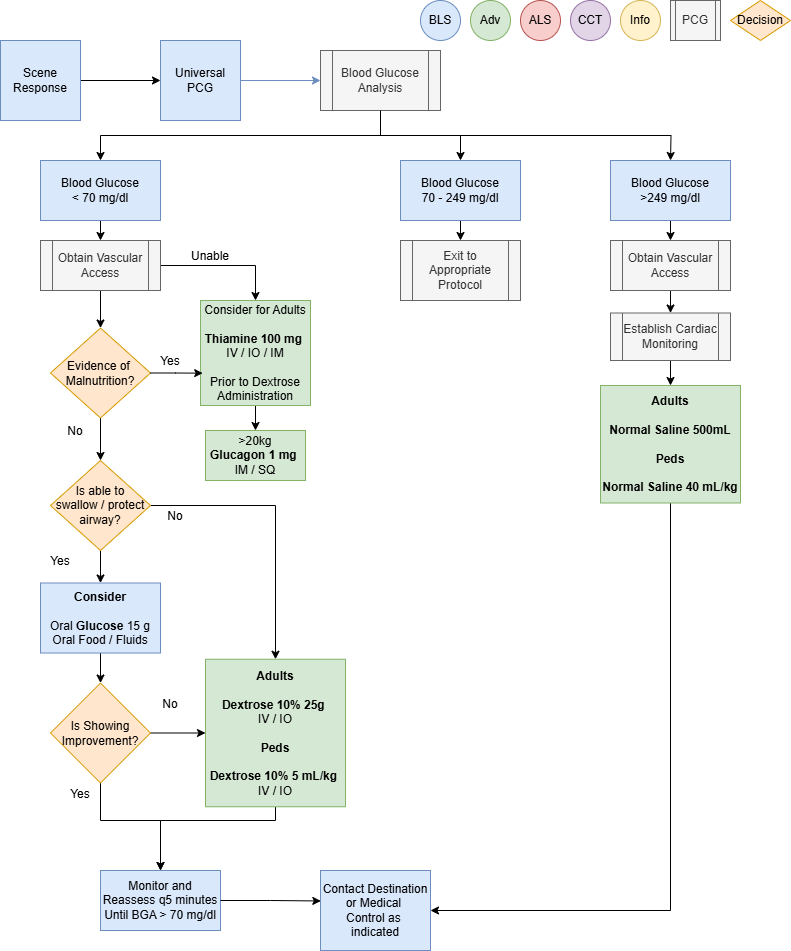
Diabetic Emergency- James Format
Applies to: Blood glucose less than 70 mg/dL or greater than 300 mg/dL and
- Patient-reported low or high blood glucose
- Diabetic patients with other medical symptoms (e.g., vomiting)
- Altered mental status
- Alcohol intoxication, suspected
- Seizure
- Stroke symptoms
- Unresponsive patients
- Cardiac arrest
Exclusion Criteria: None
BLSHistory
CheckPastbloodmedicalglucose levelhistoryIfMedications- Drug allergies
- Last Meal
- Last BGA check
Signs and Symptoms
- Altered mental status
- Combative / irritable
- Diaphoresis
- Seizures
- Abdominal pain
- Nausea / vomiting
- Weakness
- Dehydration
- Deep / rapid breathing
Differentials
- Alcohol / drug use
- Toxic ingestion
- Trauma; head injury
- Seizure
- CVA
- Altered baseline mental status
Pearls
- Patient’s refusing transport to medical facility after treatment of hypoglycemia:
- Blood sugar must be ≥ 80, patient has ability to eat and availability of food with responders on scene.
- Patient must have known history of diabetes and not taking any oral diabetic agents.
- Patient returns to normal mental status and has a normal neurological exam with no new neurological deficits.
- Must demonstrate capacity to make informed health care decisions. See Universal Patient Care Protocol UP-1.
Otherwise contact medical control.
- Hypoglycemia with Oral Agents:
- Patient’s taking oral diabetic medications should be encouraged to allow transportation to a medical facility.
They are at risk of recurrent hypoglycemia that can be delayed for hours and require close monitoring even after
normal blood glucose islessestablished. - Not
70 mg/dL, administer 10-15 grams ofall oralglucoseagentsbetweenhavetheprolongedpatient’action so Contact Medical Control or NC Poison Control Center for advice.
Patient’sgumwho meet criteria to refuse care should be instructed to contact their physician immediately and
consumecheek.a Administer additional dose of 10-15 grams of oral glucose if not improved after 10 minutes.meal.
than - Patient’s taking oral diabetic medications should be encouraged to allow transportation to a medical facility.
- Hypoglycemia with Insulin Agents
HYPOglycemia:ManyIfforms of insulin now exist. Longer acting insulin places the patient at risk of recurrent hypoglycemia even
after a normal blood glucose islessestablished.- Not
70allmg/dL,insulinsadministerhave10%prolongeddextroseactioninso50ContactmLMedical(5Controlgram)forboluses,advice. - Patient’s
minutewhoapart,meet criteria toarefusemaximumcareofshould250bemLinstructedORto25contactgramstheirofphysician50%immediatelydextrose IVP, until:the patient hasand
consume areturn to normal mental status, andthe patient’s blood glucose is at least 90 mg/dLmeal.
IfCongestive Heart Failure patients who have Blood Glucose > 250:- Limit fluid boluses unless patient has
persistentlysignsalteredofmentalvolumestatusdepletionandsuchbloodas,glucosedehydration,lesspoorthanperfusion,
hypotension,90and/mg/dLordespite treatment, repeat dosing regimen above. If unable to initiate an IV and blood glucose is less than 70 mg/dL, administer glucagon 1 mg IM/IN.If the patient has persistently altered mental status and blood glucose less than 90mg/dL at 15 minutes, transport to the hospital should not be delayed.shock.
HYPERglycemia:InIfextremebloodcircumstancesglucosewithisnogreaterIVthan/300IOmg/dL,accessadministerand10nomL/kgresponseLactatedtoRinger’sglucagon,bolusD50unlesscanrales,bewheezing,administeredpedalrectally,
Contactedema,MedicalorControlhistoryforof renal failure or CHF is present.advice.
Navigate
MCReferencesProtocols
Not Applicable
Pharmacology
- Dextrose 10%
- Dextrose 50%
- Glucagon
- Glucose
Procedures
- Vascular Access
- Limit fluid boluses unless patient has
than1